In the world of viruses, Ebola is like a chickenshit kid with a gun. Chickenshit because unlike its more deadly rivals (virals?) it hasn’t managed to evolve to be airborne – think like most hantaviruses like H1N1. With a gun, because it’s especially deadly (for a chickenshit). So deadly that it works to its own evolutionary disadvantage by wiping out its hosts quickly – too quickly. Usually devastating whole rural villages and then limping back into obscurity when it finds no new victims. Ebola is not new – it’s been around for a long while. I read about it first in Reader’s Digest when I was a child; about a really bad incident that terrorized rural Congolese villages sometime in 1976. In every case that I am aware of, Ebola burnt through the population and then ran out of steam. And its’s been usually confined to remote, forest adjacent villages.
But what we have right now is entirely new. Ebola has finally jumped the rural-urban border into the hot, dense cities of West Africa*. One of the chief features of these cities is pretty terrible health infrastructure. Being African myself, it’s still hard to fathom how vulnerable people are to health issues, how non-existent health insurance is, how woefully inadequate health institutions are, and how utterly at the mercy of disease most people are. I’ve had family members expire prematurely because of terrible hospital care, a misdiagnosis or even simply superstition (that made getting healthcare much tougher).
So a disease that is ordinarily chickenshit and should be fairly easy to control in a place with decent healthcare management systems, is loose in urban Africa. Lagos alone has over 20 million people packed into it pretty tightly. The implied epidemiology of Ebola (that I am aware of) means that it will have willing hosts and high probabilities of transmission in an urban setting that is not decisively controlled by healthcare authorities. This very weakness will also mean that the population will have to take it upon themselves to do their own protection, changing everyday activities like shop keeping, buying and selling, sex, and other mundane activities. Basically sowing grave distrust into mere commerce and everyday existence which requires human contact. Someone should be calculating the economic damage, right about now.
I am not aware of any active viral disease that has been managed successfully in an urban setting in Africa without deploying vaccines. When I was growing up, the most reliable solution to the most terrible scourges (Yellow fever, Mumps, Measles, Polio, etc.) was to get everyone vaccinated. African countries can usually handle that. It’s a one-time investment, almost latent and means that you can come into contact with the disease with relative impunity. And if you didn’t get vaccinated, oh well; you were warned sucker! Given that Ebola requires active management of a kind that may be scarce, one struggles to see how it can be cleanly wiped out in the absence of a vaccine.
If all this stuff is true (ok, big if), one plausible scenario is that Ebola becomes a low grade urban disease, never actually being wiped out, occasionally offering the illusion of complete control, but jumping out of blind corners to claim a handful of lives every few weeks and managing to soldier on. Combine that with the possibility of rapid evolution and mutation (now that is has more room to stick around), you have possibly unprecedented potential.
The debate over Zmapp – the experimental Ebola drug – has been kind of annoying, if misguided. Of course West Africans should have Zmapp, stat! Really, how much more valuable is an American or European life than an African one? The only real gate, which honestly is one that has to be self-assessed by African countries, is whether they have a health care system that can handle its efficient distribution given its high requirements for preservation in transit and administration. And if any pharma house wants to profit off a pandemic, I’d like to see them try. Regardless if I was premier in any West African country I would be setting aside a lot of money to improve health care systems, buy Zmapp and push for a vaccine. This stuff may be sticking around.
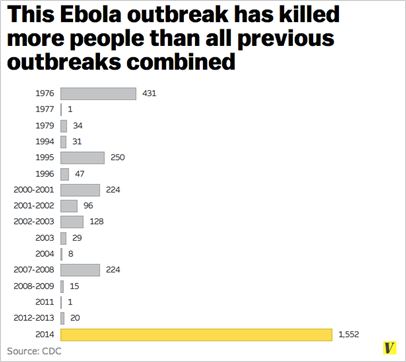
Courtesy of Vox media
*This by the way, should have been entirely predictable.
